A telemedicine ad click runs $4.50 to $7.00 in most states. So borrowing the 3 to 5 percent of revenue the clinic down the street spends leaves a telehealth practice broke by week two. The percentage looks responsible. The empty calendar disagrees.
You’re paying to reach patients across a whole state, sometimes a whole country, against competitors who do the same. Add the work of teaching people that a video visit is real care, and the cost to win one patient climbs fast. So the budget climbs with it.
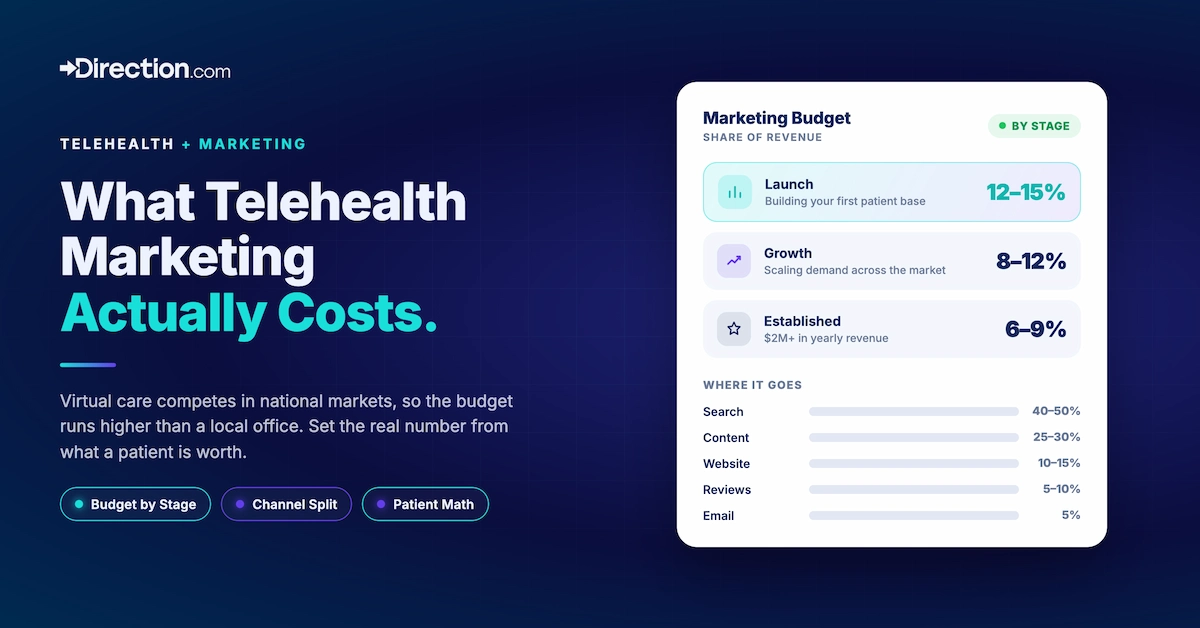
Quick answer. During startup and growth stages, 12%-15% of revenue (or more if you can swing it) should be spent on marketing. After you’ve reached $2M+/yr in revenue, 6%-9% should be enough to steadily grow as you take from the marketing budget to other parts of the company that are needed for scaling.
Set the real number from patient unit economics, meaning lifetime value and acquisition cost. Borrowing a brick-and-mortar percentage gets you the wrong starting point.
Key Data For Telehealth Marketing Budgets
- Telehealth runs higher than the 3 to 5 percent local practices spend. You compete in national markets and pay to teach patients that virtual care works.
- Budget from the math behind a patient. If a patient is worth $1,800 and you can book one for $200, you spend until that stops working.
- By stage. 12 to 15 percent of revenue at launch, 8 to 12 percent while growing, 6 to 9 percent once established.
- By channel. 40 to 50 percent search, 25 to 30 percent content and patient education, 10 to 15 percent website and booking, 5 to 10 percent reviews, 5 percent email.
- Telemedicine and prescribing advertisers need LegitScript certification before Google will run their ads.
- Search pays back in 30 to 60 days. Content and AI search take 3 to 6 months, so fund both and judge them on different clocks.
What Does Your Telehealth Marketing Budget Pay For?
Your marketing budget is the money you spend to book a virtual visit with someone who has never met you. Search ads, the website, the content that answers patient questions, the system that asks happy patients for a review. Anything that turns a stranger into a booked appointment.
One exception. Your video platform, scheduling software, and HIPAA-compliant tooling belong in operations.
People mix the two, then think they spend 20 percent on marketing when half of that line is software. Keep the columns apart or the math lies to you.
Why Virtual Care Costs More to Market Than a Local Office
A neighborhood dentist competes with a few practices inside a 10-mile radius. You compete with every telehealth brand a patient can reach from the couch.
Three things push the cost per patient up. You’re buying patients across a whole state, sometimes the whole country, where a local office buys one zip code.
People still need convincing that a video visit is real care, a job a neighborhood office never faces. And the ad space runs at premium prices on top of all that.
These prices climb fast. Search costs rose for 56 percent of healthcare advertisers last year, per LocaliQ’s 2026 healthcare benchmarks. Google now fields over a billion health searches a day.
Large hospital systems keep raising their bids, so the auction only gets steeper. The high-intent telehealth keywords I pull sit at the top of that range, $4.50 to $7.00 a click.
The teaching cost is just as real. A JAMIA Open scoping review catalogued the barriers that keep patients off telehealth. Doubt about whether virtual care measures up runs through the patient-side findings.
A neighborhood office never spends a dime to clear that doubt. You spend it on every click.
The old healthcare benchmark falls apart here. A 3 percent budget works fine when patients already drive past your building every day. Fighting for a whole state on that same 3 percent leaves you underfunded from the start.
Build the Budget From Patient Math
The revenue percentage is a starting guess. The number comes from two figures every practice can pull from its own books.
Lifetime value (LTV) is what an average patient is worth across the time they stay with you. Add up the revenue from their visits over 12 to 24 months, then add the patients they refer.
Acquisition cost (CAC) is simpler. It’s your total marketing spend in a period divided by the new patients you booked in it.
We hold to one rule with healthcare clients. Keep CAC under 20 to 25 percent of LTV, and you’ve got room to spend.
If a patient is worth $1,800 and you book one for $200, that’s a 9 to 1 return. A return like that is begging you to spend more. So you do, right up until the next patient gets expensive enough to pull the ratio back down.
The method runs in this order. The arithmetic is the easy part. Knowing which of these numbers a practice has wrong is what takes reps.
- Average revenue per telehealth patient over the last 12 months.
- Plus referral value, the patients each happy patient sends you. That total is your LTV.
- A target CAC at roughly 20 percent of LTV.
- Target CAC times the new patients you want each month. That’s your floor budget.
Two of these are where we see new clients slip. The referral number is usually a guess when we bring a practice on. And the acquisition cost leaves out leads that never booked, so it reads far healthier than the truth.
Get those two wrong and every number after them is off. Done right, the method ties your budget to a real growth goal.
Say a practice wants 40 new patients a month at a $200 CAC. That’s $8,000 in working marketing spend, whatever percentage of revenue it comes to.
Telehealth Revenue Ranges by Stage
The math sets your real budget. The percentages below tell you whether that number is sane for where your practice is. We see these ranges hold across virtual-care clients.
| Stage | Share of revenue | Why it lands here |
|---|---|---|
| Launch (first 12 months) | 12 to 15% | No referral base, no organic traffic, paying full price to teach the market you exist |
| Growth (years 1 to 3) | 8 to 12% | Some channels start working, so you scale the winners and trim the rest |
| Established (3+ years) | 6 to 9% | Referrals and organic search carry a chunk of new patients, so paid spend works less hard |
Set those ranges against the wider market. Gartner’s 2025 CMO Spend Survey put the average company at 7.7 percent of revenue, and the Duke-run CMO Survey put it near 9.4 percent. Gartner’s Ewan McIntyre called even 7.7 percent a level that “falls short for many CMOs.”
A neighborhood practice gets to run at 3 to 5 percent, since referrals and walk-by familiarity do half the work. You run higher, because every new patient starts from zero local trust, every single time.
The day your organic traffic and referrals fill a third of the schedule on their own, the percentage can come down. Until then, underspending is the fastest way to lose patients to a competitor who did the math.
Which Channels to Divide Marketing Budget Across
Once you know the number, where does it go? We start a telehealth client on the breakdown below, and it changes by specialty (more on that shortly).
| Channel | Share of budget | What it buys | When you see it work |
|---|---|---|---|
| Search (SEO and Google Ads) | 40 to 50% | The patients already searching for a provider right now | Ads in 30 to 60 days, SEO in 4 to 8 months |
| Content and patient education | 25 to 30% | Trust, and answers to the questions that stop people from booking | 3 to 6 months, then it compounds |
| Website and booking | 10 to 15% | A site that turns visits into booked appointments | Right away, every channel runs through it |
| Reviews and reputation | 5 to 10% | The third-party proof a stranger trusts more than your homepage | 60 to 90 days as reviews build |
| Email and retention | 5% | Repeat visits and referrals from patients you already won | Ongoing, the cheapest revenue you've got |
Search earns the biggest slice because intent lives there. Someone typing “online therapist who takes my insurance” is closer to booking than anyone you reach on social. Search is also where strong telehealth marketing campaigns really come in.
Patients now ask ChatGPT, Perplexity, and Google’s AI Overviews for provider recommendations, and those tools cite the pages they trust.
Earning those citations is a process of its own, and it’s built into our telehealth SEO campaigns.
Inside any one channel, the 70/20/10 rule keeps you from betting the whole budget on a hunch. Put 70 percent into what already books patients, 20 percent into channels showing early promise, and 10 percent into a test you’re unsure about. That keeps most of your money on what works while funding the search for the next winner.
Example for a Practice at $50k/Month in MRR
This is typically the growth stage. So, I recommend $5,000 a month at minimum should be going to marketing.
| Channel | Monthly spend | What it covers |
|---|---|---|
| Search (SEO and ads) | $2,250 (45%) | Google Ads for virtual visits, plus SEO for the conditions the practice treats |
| Content and education | $1,400 (28%) | Articles and FAQs that answer patient questions and earn AI citations |
| Website and booking | $650 (13%) | Conversion fixes to the booking flow |
| Reviews | $450 (9%) | A system that asks every patient for a review after the first visit |
| $250 (5%) | Retention and referral prompts |
At a $150 to $200 acquisition cost, $5,000 books roughly 25 to 33 new patients a month. A booked patient runs more than a raw web lead, so that range stays healthy against an $1,800 patient value.
If each is worth $1,800 over their time with the practice, that month of spend ties to $45,000 to $59,000 in lifetime revenue. That’s the return you protect by holding steady through the first slow week.
The Google Ads Rule That Changes Your Telehealth Marketing Budget
Before writing this, I read a dozen budget guides and didn’t see this rule in a single one. That’s the scary part, because I’ve seen it freeze a telehealth account overnight.
Google’s healthcare advertising policy makes telemedicine and prescription-drug advertisers get certified through LegitScript before a single ad runs. No certification, no ads.
The certification itself takes weeks and a fee, so it goes in the launch budget before a single ad runs.
Then there’s the risk cost. Google runs a strike system, and health ads get flagged by review filters that don’t always get it right. One careless campaign can suspend the account.
What does that mean for the budget line? Put paid search in the hands of someone who runs healthcare accounts.
A generalist learning your rules on your dime? That’s how accounts get suspended. The fee for someone who knows the healthcare ad rules well is far cheaper than a banned account and an empty calendar.
Budget Differences by Specialty
The framework holds across virtual care. The emphasis moves with what your patients need to hear before they book.
Mental health. Stigma and privacy fears slow the decision, so the content and education slice carries more weight.
Paid search bites hard here too. The cost of a mental-health click jumped over 42 percent in a year. The average lead now runs $141, the highest in healthcare, per LocaliQ.
People read three or four articles before booking a first therapy session, so be the source of all four.
Urgent and same-day care flips the priorities. Intent is immediate. Paid search takes the bigger share, because someone with a sinus infection at 9 p.m. isn’t reading your blog. They click the first ad that promises a visit tonight.
Primary and chronic care. Here the money sits in keeping patients, which pushes email and retention up the list. A managed-condition patient who stays two years is worth more than three one-visit patients, and costs far less to keep.
How to Tell If Your Telehealth Marketing Budget Is Working
Marketing you can’t measure is marketing you overpay for. Three numbers inform you on whether the spend is working or not.
In The CMO Survey, demonstrating marketing’s impact on financial outcomes has ranked as the top challenge for marketing leaders. A telehealth practice keeps marketing accountable by tying every dollar to a booked patient.
- Acquisition cost per channel, broken out by source. It’s the number that shows which channel books patients for what you pay.
- LTV to CAC ratio. Patient value over acquisition cost (above 3 to 1 is healthy, above 6 to 1 says spend more).
- Payback period. The months a patient takes to earn back what you spent winning them, with under six on paid channels as the target.
The discipline is simple to describe and hard to keep. Every channel earns 90 days to book patients at an acceptable cost, and the ones that miss lose their budget to the ones that hit.
That call gets made monthly, on the data. Run it on gut feel a few times a year, and a practice ends up funding the channel that flatters it. Consistency is what makes it work, and it’s the first thing to slip when budget management is one more job on an owner’s desk.
For a deeper read on the percentage question, our breakdown of the right percentage of revenue to spend on marketing goes channel by channel.
What Expert Execution Buys You
Everything above is the setup. I’ve watched telehealth practices burn through cash on a dozen scattered tactics. I’ve watched others book a full schedule on half the money because they spent it right.
The difference came down to one thing. Somebody read the numbers every month. They moved money toward whatever was booking patients and pulled the slow channel before it drained the quarter.
At Direction, we outline the plan before a practice signs anything. We focus on the math from spend to booked patients, with the budget tied to your LTV and CAC.
Want to review your current marketing budgets performance? Book a discovery call with the Direction team.
Common Telehealth Marketing Questions
What's a reasonable telehealth marketing budget?
For a virtual-first practice, 12 to 15 percent of revenue at launch and 6 to 9 percent once established. The exact figure should come from your patient lifetime value and acquisition cost.
What if I can't afford the recommended percentage?
A smaller budget works when you pour it into one channel. For a telehealth practice that’s usually search, where buying intent runs highest. The judgment is in picking the right channel for your specialty and holding off on the rest until it pays. That’s the call a specialist makes daily, and a stretched owner rarely lands it alone.
How quickly should expect to see results?
Google Ads can book patients in 30 to 60 days. SEO and content take 3 to 6 months to build, then keep paying without the per-click cost. Fund both, and judge each on its own clock so you don’t kill a slow channel that’s about to compound.
Do seasonal swings change the budget?
Patient volume rises in winter and dips in summer for practices treating seasonal conditions. Spend tends to run heavier from October through March and lighter from May through August. A mental-health or dermatology practice often follows a different curve, I’d confirm against booking data first, though.